Primitive Torsion of the Omentum: A Case Report
Article Type
Case Report
Online Date
May 07, 2025
Open Access
Yes
Michela Carmela Scollica*, Amedeo Elio
Department of General Surgery, San Bonifacio Hospital, Verona, Italy
*Corresponding author: Michela Carmela Scollic, Department of General Surgery, San Bonifacio Hospital, Verona, Italy
Citation: Scollica MC, Elio A (2025) Primitive Torsion of the Omentum: A Case Report. Glob J Surg Surgical Res 1(1): 29-32.
Received Date: 15 April 2025; Accepted Date: 05 May 2025; Published Date: 08 May 2025
Introduction
Torsion of the omentum is a rare and unusual cause of abdominal pain in adults and children. It is very difficult to make a correct preoperative diagnosis from a clinical point of view, because this condition can mimic symptoms attributable to other acute abdominal pathological manifestations. Omental torsion can be primary or secondary to pre-existing abdominal pathologies. It mainly affects adults, male and often overweight. Many cases are diagnosed intraoperatively and treated by omentectomy.
Case Report
We present the case of a 26-year-old girl, normotype, normal weight, who arrives at the emergency room for a symptomatology characterized by abdominal pain localized mainly in FID, which arose the previous evening, associated with fever. She negates nausea and/or vomiting. The patient enjoyed excellent health, did not report previous surgeries and major pathologies. Negative history of trauma. The menstrual cycle was regular and she denied recent sexual intercourse. Not taking oral estroprogestin therapy. The patient, during the visit, was pyretic and hemodynamically stable. The abdomen was treatable, unstretched, with pain localized in the right iliac fossa associated with peritoneal irritation. The blood chemistry tests performed were normal, not detecting an increase in GB, but a slight increase in PCR 29. The HCG beta test was negative. The complete abdomen ultrasound carried out had shown that FID recognized a tubular structure with a blind bottom, slightly distended, with an AP diameter of about 6 mm and coexistence of slight hyperechogenicity of the surrounding adipose tissue (Figure 1). It was recognizable slender fluid aquifer in FID and in small basin. The patient had also undergone a gynecological examination with transvaginal ultrasound that had not shown alterations in the uterus and annexes. In the light of the clinical and instrumental picture, an indication was given for urgent exploratory laparoscopy in the suspicion of acute appendicitis. Laparoscopy showed the presence of blood fluid in Douglas. Annexes in the norm, as well as the appendix that did not show signs of inflammation. Negative research of Meckel's diverticulum and other abdominal pathological conditions. It was noted the presence of torsion of the great omentum, necrotic in its distal tract for about 5 cm, with pedunculated appearance and localized in the right para-ovarian site (Figure 2). It was therefore proceeded to a section of the same by bipolar gripper. The post-operative course was regular and the patient was discharged on the 2nd post-operative day in good general clinical condition. Histological examination of the surgical piece confirmed the presence of chronic inflammation and hemorrhagic infarction of the omental portion.
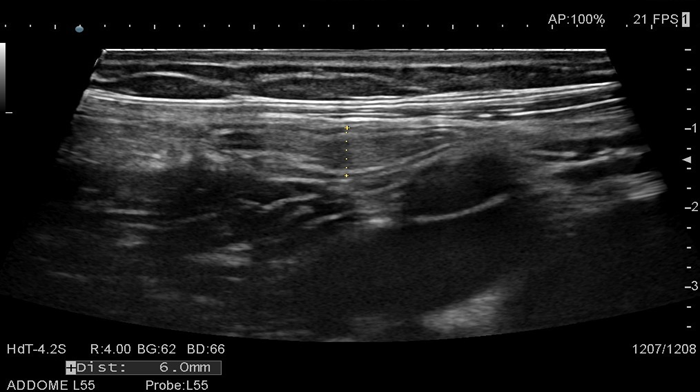
Figure 1: Preoperative abdomen ultrasound that recognized a tubular structure with a blind bottom with an AP diameter of about 6 mm and coexistence of slight hyperechogenicity of the surrounding adipose tissue.
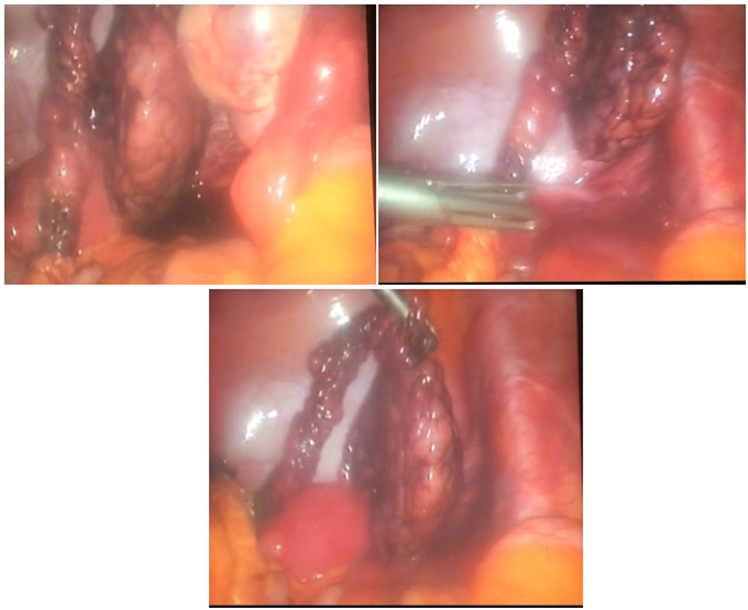
Figure 2: Intraoperative findings- Presence of torsion of the great omentum, necrotic in its distal tract for about 5 cm, with pedunculated appearance and localized in the right para-ovarian site.
Discussion
Torsion of the great omentum is an uncommon cause of acute abdomen, accounting for about 1.1% of all abdominal pain cases [1]. Its preoperative diagnosis is difficult by simulating thick acute pictures represented by appendicitis and cholecystitis [2-5]. A review of the literature, considering the data available on search engines [6,7], has shown that this condition affects more the male sex than the female one with a ratio of 2: 1 and affects mainly between 20 and 50 years [8]; this condition is also frequent in pediatric age [9-12]. Omental torsion is classified in SECONDARY, when linked to factors such as: previous surgery, abdominal inflammatory processes [13], hernial pathology , benign or malignant tumors [14-16]. It is defined, instead, PRIMITIVE (in a 1/3 of the cases), when linked to predisposing factors such as obesity (for irregular distribution of fat), anatomical variations (bifid- omentum [17], accessory and pedunculated omentum [18] and vascular anomalies) and / or precipitating factors such as trauma [19] and sudden changes in body position [1] that cause a significant increase in abdominal pressure. The diagnosis is in most cases intra-operative, but it has been shown that the use of diagnostic methods such as ultrasonography and computed axial tomography is able to diagnose suspicion thanks to the radiological aspect that omental fat can assume. Ultrasound often shows a hyperechoic mass or structure, not compressible at the site of pain. On the other hand, the CT scan shows an inflammatory focal mass with adipose density with the appearance of linear and swirling structures typical of vascular torsion [20,21]. Percentage, the preoperative radiological diagnosis of omental torsion is far lower than the diagnosis of other inflammatory diseases, first of all acute appendicitis. Blood chemistry tests often do not show noteworthy alterations except for a non-significant increase in inflammation indices and clinically pain can occur acutely, subsequently presenting continuity, persistence and in many cases worsening or even intermittency. Pain is localized to the right quadrants in almost all the cases described in the literature and in particular in the right iliac fossa [22-24], but in some cases it can be spread or even localized to the upper quadrants simulating pictures of cholecystitis and / or masses not better defined as described by Scabini et al [25]. It all depends on the site of localization of the portion of omentum [26]. Treatment is surgical. Exploratory laparoscopy is the most widely used technique with removal of the portion of omentum affected by torsion [27,28]. It is fair to underline that in the literature, conservative treatments [29] have also been reported, with positive outcome and complete resolution of the symptoms and the intra-abdominal picture as well as conservative attempts with negative results as described by Kataoka et al [13]. In light of all this, an accurate use of diagnostic techniques could lead to the diagnosis of omental torsion. However, surgery is critical for certainty diagnosis and treatment. In our case the precipitating factors described and favoring the appearance of this pathological condition are not present, therefore we can say that even today, despite the existing publications, all the conditions that can give rise to primitive omental torsion are not fully known [30]. Undoubtedly it is essential that this, although rare, is considered in the differential diagnosis with other pathological conditions especially when imaging, laboratory data and the clinic are not the prerogative of a given acute abdominal pathology. However, surgical treatment that provides diagnostic confirmation and treatment remains fundamental.
Conclusion
Omental torsion, although still considered a rare cause of acute abdominal pain, should be included in the differential diagnosis especially of FID pain. Preoperative diagnosis is difficult and surgery is considered the treatment of choice.
References
- Camilla Cremonini, Andrea Bertolucci, Dario Tartaglia, Francesca Menonna, Christian Galatioto, et al. (2016) Acute abdomen caused by greater omentum torsion: A case report and review of the literature- Ulus Travma Acil Cerrahi Derg 22: 4.
- Hiyad Al-Husaini, Aidelole Onime, Soji F. Oluwole (2000) PRIMARY TORSION OF THE GREATER OMENTUM- J NatI Med Assoc 92: 306-308.
- Konstantinos Alexiou, Argyrios Ioannidis, Ioannis Drikos, Nicolaos Sikalias, Nicolaos Economou (2015) Torsion of the greater omentum: two case reports- Journal of Medical Case Reports 9: 160.
- Syed Danish Ali, Syed Sheeraz-ur-Rahman (2013) Common presentation uncommon diagnosis Primary Omental Torsion- Case report 63.
- Rahul Gupta, Waad Farhat, Houssem Ammar, Mohamed Azzaza, Sami Lagha, et al. (2019) Idiopathic segmental infarction of the omentum mimicking acute appendicitis: A case report. International Journal of Surgery Case Reports 60: 66-68.
- Vijay Borgaonkar, Sushil Deshpande, Mukesh Rathod, Imran Khan (2013) Primary Omental Torsion Is a Diagnostic Challenge in Acute Abdomen-a Case Report and Literature Review-Indian J Surg 75: 255-257.
- Nina Breunung, Paul Strauss (2009) A diagnostic challenge: primary omental torsion and literature review - a case report- World Journal of Emergency Surgery 4: 40.
- Alin Mihe?iu, Alexandra Sandu, Dan Bratu, Cristina Mihe?iu (2021) Laparoscopic Management of Primary Omental Torsion- Case Reports in Surgery 6.
- Anyfantakis D, Kastanakis M, Karona V, Symvoulakis EK, Fragiadakis G, et al. (2014) Primary omental torsion in a 9 year old girl: a case report- Journal of Medicine and Life 7: 220-222.
- Chijioke Chinaka, Shahbaz Mansoor, Mohamed Salaheidin (2018) Torsion of the Omentum: A Rare Cause of Acute Abdomen in a 14-Year-Old Boy- Hindawi Case Reports in Surgery 2018.
- Khattala Khalid, Tenorkorang Snr Somuah, Elmadi Aziz, Rami Mohamed, Bouabdallah Youssef (2013) Primary omental torsion in children: case report. Pan African Medical Journal 14: 57.
- Elham Khalili, Mahdis Marashi, Majid Safarpanah, Saeedeh Majidi, Zahra Ghaeini Hesarooeyeh (2022) Omental torsion mimicking acute appendicitis in a 7-year-old boy: a case report-Journal of Medical Case Reports 16: 286.
- un Kataoka, Toshikatsu Nitta, Masato Ota, Yuko Takashima, Yuta Yokota, et al. (2019) Laparoscopic omentectomy in primary torsion of the greater omentum: report of a case- Surgical Case Reports 5: 76.
- Yousuke Kinjo, Yasushi Adachi, Kunihiko Seki, Michihiko Tsubono (2014) Laparoscopic resection for torsion of an omental lipoma presenting as an acute abdomen in a 5-year-old gir 2014.
- Chjoong Howe Alvin Tani, Bernard Chi Shern Hoe, Vishalkumar Shelat, Cher Heng Tani (2012) Leiomyomatosis peritonealis disseminata presenting as omental torsion. Singapore Med J 53: 71-73.
- Marcos Sforza, Katarina Andjelkov, Dejan Ivanov, Zoran Mari?i?, Slobodan Krsti? (2012) A Rare Case of Benign Omentum Teratoma- Srp Arh Celok Lek 140: 362-364.
- Vicky Dhooghe, David Reynders, Peter Cools (2016) Torsion of a bifid omentum as a rare cause of acute abdomen: a case report- Journal of Medical Case Reports 2016.
- Tareq M. Al-Jaberi, Kamal I. Gharaibeh, Rami J. Yaghan (2000) TORSION OF ABDOMINAL APPENDAGES PRESENTING WITH ACUTE ABDOMINAL PAIN- Annals of Saudi Medicine 2000.
- Mehrdad Hosseinpour, Azadeh Abdollahi, Hoda Jazayeri, Hamid Reza Talari, Ahmad Sadeghpour (2012) Omental Torsion After Repeated Abdominal Blunt Trauma- Arch Trauma Res 2012: 1.
- Michael Karanikas, Konstantinia Kofina, Ferdi Boz Ali, Vasileia Vamvakerou, Eleni Effraemidou, et al. (2018) Primary greater omental torsion as a cause of acute abdomen-a rare case report-Journal of Surgical Case Reports 8: 1-3.
- Mustafa Kerem, Abdulkadir Bedirli, B. Bulent Mentes, Omer Sakrak, Ilker Pala, et al. (2005) Torsion of the Greater Omentum: Preoperative Computed Tomographic Diagnosis and Therapeutic Laparoscopy- JSLS 9: 494-496.
- A Kumar, J. Shah, P. Vaidya (2016) Primary omental gangrene mimicking appendicular perforation peritonitis-A case report- /International Journal of Surgery Case Reports 21: 67-69.
- Kamal Sanjiva Hapuarachchi, Edward Douglas Courtney, Szabolcs Gergely, Tjun Yip Tang (2009) Torsion of parietal-peritoneal fat mimicking acute appendicitis: a case report. Journal of Medical Case Reports 3: 6980.
- Ghosh Y, Arora R (2014) Omental Torsion. Journal of Clinical and Diagnostic Research 08: NE01-NE02.
- Stefano Scabini, Edoardo Rimini, Andrea Massobrio, Emanuele Romairone, Chiara Linari, et al. (2011) Primary omental torsion: A case report. World J Gastrointest Surg 3: 153-155.
- Hideki Katagiri, Kunpei Honjo, Motomi Nasu, Minoru Fujisawa, Kuniaki Kojima (2013) Omental Infarction due to Omental Torsion. Case Reports in Surgery 2013.
- Ha JPY, Tang CN, Siu WT, Tsui KK (2006) Laparoscopic Management of Acute Torsion of the Omentum in Adults. JSLS 10: 351-354.
- Ali Tasleema, Qamar Zamana, Daniel A Thomasa, John G Paynea, Rajab Kerwata, et al. (2013) Omental Torsion: An Unusual Cause of Right Iliac Fossa Pain and Role of Laparoscopic Management. Gastroenterology Research 6: 237-239.
- Mohhamad-Hadi Saeed Modaghegh, Reza Jafarzadeh (2011) Primary Omental Torsion in an Old Woman: Imaging Techniques Can Prevent Unnecessary Surgical Interventions. Case Reports in Medicine 2011.
- Shivani Joshi, Gary Andrew Cuthbert, Rajab Kerwat (2016) Omental torsion, a rare cause of acute abdomen- BMJ Case Rep 2016.