“Successful Microsurgical Replantation of Near-Total scalp avulsion in a teenager-A Case Report”
Article Type
Case Report
Online Date
March 03, 2025
Open Access
Yes
Bhagyashri Talele1*,Nikhil Agarkhedkar2, Shravani Shetye2
1Department of Plastic Surgery, Deenanath Mangeshkar Hospital, Erandwane, Pune, India
2Department of Plastic Surgery, Deenanath Mangeshkar Hospital, Pune, India
*Corresponding author: Bhagyashri Talele, Department of Plastic Surgery, Deenanath Mangeshkar Hospital, Erandwane, Pune, India
Citation: TaleleNikhil B, Agarkhedkar N, Shetye S (2025) “Successful Microsurgical Replantation of Near-Total scalp avulsion in a teenager-A Case Report”. Glob J Surg Surgical Res 1(2): 65-69.
Received Date: 15 May 2025; Accepted Date: 20 July 2025; Published Date: 01 August 2025
Introduction
Entire avulsion of the scalp is an infrequent disfiguring injury caused by severe shearing forces to the hair-bearing scalp 1. It has usually been associated with entanglement of the hair in rotating machinery [1]. Long hair worn increases the hazard of descalping injuries [2]. Microsurgical replantationis the primary treatment for total scalp avulsion, depending on factors like scalp availability, ischemia time, and vessel viability [3]. The refinement of microvascular techniques has made the replantation of amputated scalp possible. Wepresent a case of a 14 year old girl withnear-total scalp avulsion caused byher hair caught in a rotating sugarcane crushing machine.
Clinical Report
A 14 year old girl had a total scalp avulsion in November 2024. Her hair was caught in a sugarcane crushing machine (Figure 1A&B).
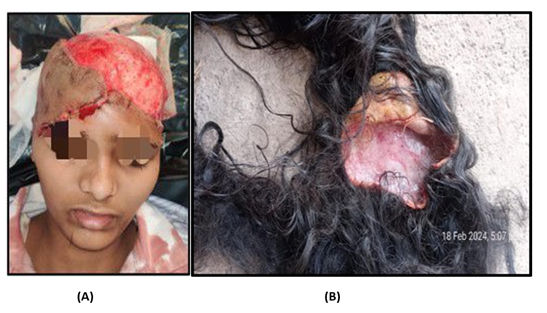
Figure 1: A: Pre-operative injured head on admission.; B: Avulsed scalp with long hair.
The patient presented to theemergency room of ourhospital 3 hours after the injury. The avulsed scalp was abandoned by the patients relativesat the location of trauma. The patient was primarily attended in the emergency room. She did not give any history of loss of consciousness or bleeding through ear or noseor blurring of vision. Fluid resuscitation was done to prevent hemorrhagic shock.Broad spectrum Intravenous antibiotics were administered. Clinical examination was performed to rule out other systemic injuries such asintra cranial injury ,any bony fractures ,cervical spine injury etc. There was near total avulsion of scalpinvolving left temporoparietalandright parieto- occipitalregion. There was a contused lacerated wound over the right frontotemporal region splitting the eyebrowanteriorly. Laboratory tests-Complete Blood counts, Renal Function Tests, Liver Function Tests and Coagulation Profile werewithin normal limits. Informed consent for surgery was obtained from the patients parents. The patient was immediately shifted to the Operating roomfor exploration and meanwhile the father of the patient was asked to procure the avulsed scalp from the site of incidence.
Operation Procedure
In the operating room , pt was placed in supine position. Endotracheal intubation was performedand the surgery was performed under General Anesthesia. Thorough lavage was given with normal saline solutionand debridement of unhealthy tissues and debris was done (Figure 2).

Figure 2: Intra- operative photos of the native scalp after debridement and lavage. Right eyebrow wound was repaired in layers.
Left superficial temporal artery and vein were identifiedand crushed ends were trimmed and prepared for microvascular anastomosis under microscope. The right Superficial artery and vein were part of the degloved skin. Hence, were not available for anastomosis. Meanwhile , another team (on the bench) prepared the amputated part ofavulsed scalp. The amputated part waslaid over around utensil for preparation. Trimming of hair, removal of debris, debridement of unhealthy tissues followed by thorough lavage with normal salinewas done. Under microscopic magnification-exploration was done to identify Superficial Temporal Artery and Vein andwere prepared for anastomosis. End to end arterial and venous anastomosiswas done withmonofilament nylon 10-0 in interrupted fashion. The reimplanted scalp showed bright red bleeding from the edges. The operative time was 6 hours, 30 minutes. The scalp segments were sutured with nylon 3-0. Vacuum drainage tube was placed under the replanted scalp.Hand held doppler was used to confirm the satisfactory blood flow in the replanted scalp. The dressing of the operated sitewas done with loose bandage with a window created using gauze pads to monitor the replanted scalp.
Post- operatively patientwas shifted to ICU for closed monitoring of vitals . Hourly monitoring of replated scalp was done – its color , bleeding on pin prick and doppler signals were noted. No significant problem in the arterial or venous blood flow was noted in post operative period.Patient was shifted from the ICUto the wards on Post operative day 3 (Figure 3).

Figure 3: Photo of patient on Post operative day 7 showing viable replanted scalp with necrotic zone at frontal stitchline.
Patient was discharged from the hospital on Post operative day 7. Post which patient followed up on outpatient basis .Sutures were removed on Post operative day 15. Segmentary Focalpartial thickness necrosis was observed in the occipitalandparietal region and these regions healed secondarily (Figure 4 A&B).
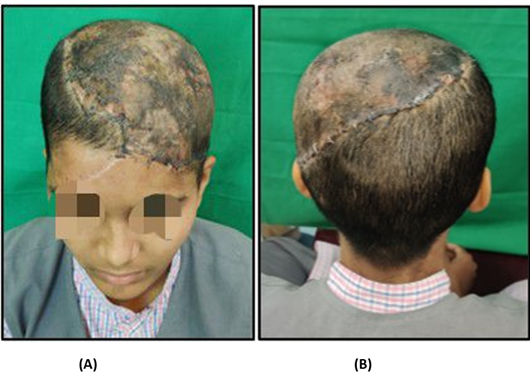
Figure 4 : A and B - Front and Back viewon Post operative day 15 showing zones of segmental necrosis.
Discussion
Scalp avulsion injuries usually occur following hair entrapment in machinery. The full-thickness avulsion usually starts in the supraorbital and nuchal areas because the frontalis and occipitalis muscles present less resistance than the galea [4]. Replantation is the best form of reconstruction following total avulsion of the scalp. If the scalp is not replanted, the patients undergo skin grafting of the raw area [5]. Flap coverage followed by graft is an effective and acceptable option when replantation is not feasible3. The latissimus dorsi muscle flap is commonly employed for large scalp reconstructions due to its size, reliable vascular pedicle, and effective results when covered with a Split thickness skin graft [6] . However, reconstruction with a skin graft leads to complete alopecia and later on hair restoration is challenging and required multiple procedures. Thus , utmost efforts should be undertaken to save the avulsed scalp even in a severely damaged condition. The first successful replantation ofscalp was reported by Miller et al. in 1976 [7]. The rich vascular supply of scalpallows its irrigation by means of only one arteriovenous temporal pedicle [8]. The number of vessels anastomosed may not be the key factor for scalp survival as described byby Yin et al. [9]. However, Arashiro et al advocated that- Bilateral arterial anastomoses are more reliablefor adequate arterial flow [10]. The decision regarding the number of vascular repairs to be performed in total scalp avulsions should be based on the patient’s clinical condition at the time10. Also , at times , this is limited by the number of vessels available of micro-vascular anastomosis. The superficial temporal vessels are regarded as the most suitable vascular pedicle for scalp revascularization [11] .Liu et al also preferred the vessels in juveniles because these are of thickest diameter and less variable in the scalp since other vessels are too thin to be anastomosed and more prone to thrombosis [12]. Dr. Sabhapaty et al . advocated that-When at least two major veins are repaired, bleeding after clamp release is significantly reduced [5].
Neovascularization from the recipient bed normally contributes to the survival of a skin flap, but this is not available in a scalp flap because no blood supply to the scalp is contributed by the skull or cranial aponeurosis [13]. Warm ischemia time of the avulsed scalp is one of the important factors contributing to the success of replantation [14]. Every effort should be made to shorten the time before revascularization of the avulsed scalp. In this case, warm ischemia time had been 8 hours when anastomosis started; thus, we anastomosed the artery first to provide the avulsed scalp with blood supply as soon as possible. The two main challenges faced by us were First, the amputated part of the scalp was left behind at the place of injury and it was uncertain whether we would be able to retrieve it . But , despite that, one team had already started with exploration of the native scalpfor vessel preparation so as to reduce the warm ischemia time in case the part would be obtained.Another challenged was-when the amputated part was received, it was highly contaminated with debrisand it was a very big challenge to clean the part. Hair once struck on the inner surface is very painstaking to remove and makes the surgery difficult by mimicking the 10.0 nylon used for tagging of the vessels [5].
The segmental areas of necrosis which heal with secondary intention develop alopecia. Other factors responsible foralopecia are the warm ischemia time and the physiological shock to the hair follicles. Such areas of alopecia can be dealt with by camouflaging by hairstyle or may be excised and replacedwith pre-expanded rotational flaps from hair bearing areas [15]. In our case , the centralmost area of the replanted scalp developed alopeciawith patches of hair growthat follow up at14 months .The patient is currently receiving medical management for alopecia (Figure 5 A&B).
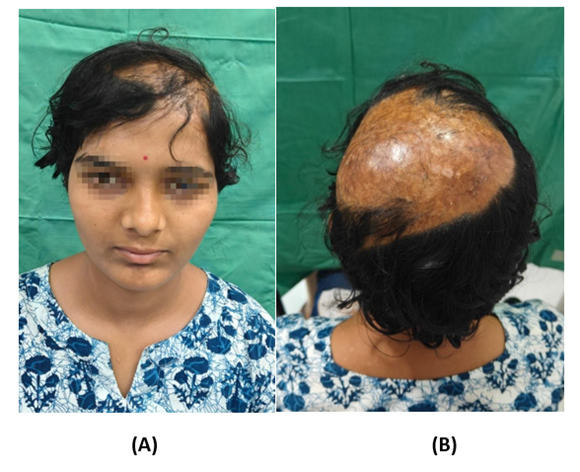
Fiqure 5: A and B show front and back viewat followup at 14 months showing central zone of alopecia.
Although there are many primary or secondary reconstructive options for reconstruction of scalp defect after scalp loss , efforts must be made to save the avulsed scalp and attempt a microvascular re-implant whenever possible in order to reduce lifelong disfigurement.
References
- Arashiro K, Ohtsuka H, Ohtani K, et al. (1995) Entire scalp replantation: Case report and review of the literature. J Reconstr Microsurg 11: 245-250.
- FeierabendTC, Bindra RN (1985) Injuries causing major loss of scalp. Plast Reconstr Surg 76: 189.
- Paudel S, Luitel P, Thapaliya I, Thapa A, Sharma S (2024) Successful management of severe scalp avulsion injury: a case report and review of surgical interventions. J Surg Case Rep 590.
- Hidalgo DA: Replantation of the scalp and ear: In Microsurgery in Trauma. NY: Fukuta Publishing 1987: 105.
- Sabapathy SR, Venkatramani H, Bharathi RR, D'Silva J (2006) Technical considerations in replantation of total scalp avulsions. J Plast Reconstr Aesthet Surg 59: 2-10.
- Rochlin DH, Broyles JM, Sacks JM (2013) Interesting case series scalp reconstruction with free latissimus Dorsi muscle. Eplasty ic53.
- Miller GD, Austee EJ, Shell JA (1976) Successful replantation of an avulsed scalp by microvascular anastomoses. Plast Reconstr Surg 58: 133-136.
- Juri J, Irigaray A, Zeaiter C (1990) Reimplantation of scalp. Ann Plast Sur 24: 354-361.
- Yin JW, Matsuo JMS, Hsieh CH, et al. (2008) Replantation of Total avulsed scalp with microsurgery: experience of eight cases and literature review. JTrauma 64: 796-802.
- Livao?lu M, Uraloglu M, Imamo?lu Y, Altun EM, Karaçal N (2016) Microsurgical Replantation of Two Consecutive Traumatic Total Scalp Avulsions. J Craniofac Surg 27: e767-e768.
- Barisoni D, Lorenzini M, Governa M (1997) Two cases of scalp reimplantation based on one artery and one vein with interposed vein grafts. Eur J Plast Surg 20: 51Y53.
- Liu T, Dong J, Wang J, Yang J (2009) Microsurgical replantation for child total scalp avulsion. J Craniofac Surg 20: 81-84.
- Preis FWB, Urzola V, Mangano A, et al. (2007) Subtotal scalp reconstruction after traumatic avulsion: A technical note. J Craniofac Surg 18: 650Y653
- Cheng K, Zhou S, Jiang K, et al. (1996) Microsurgical replantation of the avulsed scalp: a report of 20 cases. Plast Reconstr Surg 97: 1099Y1108
- Nasir S, Karaaltin M, Erdem A. (2015) Total scalp replantation. JCran-iofac Surg 26: 1192-1195.