Surgical Outcomes of Hip Hemiarthroplasty for Hip Fracture in Extremely Obese Patients
Article Type
Research Article
Online Date
April 03, 2026
Open Access
Yes
Ahmed Nageeb Mahmoud1*, Sanjum Singh2, Caitlyn Kline3, Daniel Hayes4, Daniel Scott Horwitz2
1Orthopedic Surgery Department, Faculty of Medicine, Ain Shams University, Cairo 11591, Egypt
2Geisinger Medical Center, Danville, PA, USA
3Geisinger Commonwealth School of Medicine, Scranton, PA, USA
4University of Kentucky College of Medicine, Lexington, KY, USA
*Corresponding author: Ahmed Nageeb Mahmoud, Orthopedic Surgery Department, Faculty of Medicine, Ain Shams University, Cairo 11591, Egypt
Citation: Mahmoud AN, Singh S, Bernate J, Kline C, Hayes D, Horwitz DS (2026) Surgical Outcomes of Hip Hemiarthroplasty for Hip Fracture in Extremely Obese Patients. Glob J Surg Surgical Res 2 (1):91-98.
Received Date: 16 March, 2026; Accepted Date: 27 March, 2026; Published Date: 30 March, 2026
Abstract
Background: Hip hemiarthroplasty (HA) is a common treatment for displaced femoral neck fractures in elderly patients, yet its outcomes in extremely obese individuals (BMI ≥40 kg/m²) have not been specifically reported.
Methods: We retrospectively reviewed 36 HA cases (35 patients) with BMI ≥40 kg/m² treated at a single institution. Demographics, comorbidities, surgical details, and postoperative outcomes were analyzed.
Results: The cohort had a mean age of 72.6 years and a mean BMI of 45.6 kg/m². Wound-related complications occurred in 13.9% of cases, including prosthetic joint infection (PJI) in 11.1%. Mortality was 17.14% at 3 months, 28.57% at 1 year, and 48.57% at 3 years. No cases of dislocation, periprosthetic fracture, or primary acetabular erosion were observed.
Conclusions: HA in extremely obese patients is associated with a substantial risk of PJI, while mechanical complications appear less frequent, possibly due to limited mobility. These findings underscore the need for tailored perioperative strategies and risk counselling in this high-risk population.
Keywords: Hip Hemiarthroplasty; Femoral Neck Fractures; Obesity, Morbid; Body Mass Index; Postoperative Complications; Prosthetic Joint Infection; Mortality
Introduction
Hip fractures are a significant contributor to functional decline and reduced life expectancy in older adults [1]. Studies indicate that approximately 15% to 50% of patients die within the first year following a hip fracture, with mortality rates notably higher in unstable hip fractures treated with hemiarthroplasty, which can reach as high as 32% [2-6]. Hip hemiarthroplasty (HA) is a successful treatment option for displaced femoral neck fractures in elderly patients [7-9]. A range of factors has been implicated
in the increased morbidity and mortality following HA. Patientrelated comorbidities, including elevated Charlson Comorbidity Index (CCI), peripheral vascular and cerebrovascular disease, advanced age, diabetes, obesity, renal and hepatic dysfunction, and malignancies, substantially heighten the risk of periprosthetic joint infection (PJI). Surgical considerations, such as the use of uncemented stems and procedures performed by non-arthroplasty specialists, further contribute to adverse outcomes. Additionally, postoperative elements like extended hospitalization, hematoma formation, prolonged wound drainage, and repeated urinary catheterizations have been identified as significant risk factors [10-13].
Obesity is among the recognized risk factors for poor outcomes, particularly prosthetic joint infection, after HA [13]. Obesity defined by the World Health Organization as a body mass index (BMI) of 30 kg/m² or higher, reflects excess body fat resulting from caloric surplus. It is further classified into three categories, with class III (extreme obesity) starting at a BMI of 40 kg/m². According to recent National Health and Nutrition Examination Survey (NHANES) data, over 73% of U.S. adults have a BMI above the normal range, with over 40% classified as obese and over 9% as extremely obese (with a BMI at or above 40.0 kg/m²) [14-19].
While HA is the most common treatment option for displaced femoral neck fractures in elderly patients [20], and with the high incidence of extreme obesity [19], the outcomes of HA in extremely obese patients have been seldom reported in the literature. Only one study investigated the impact of obesity on surgical and postoperative outcomes in patients undergoing hip hemiarthroplasty (HA) or total hip arthroplasty (THA) for isolated femoral neck fractures, categorizing patients by body mass index (BMI) into obese and non-obese groups [21]. The authors found obesity to be associated with significantly longer operative times in both HA and THA procedures, as well as increased total operating room time and anesthesia duration in THA. However, the authors found that postoperative complication rates did not differ significantly between obese and non-obese patients undergoing each procedure.
Given the distinct surgical considerations and patient characteristics between HA and THA, and the wide variability in obesity severity, this retrospective study aims to examine outcomes in a specific cohort of extremely obese patients undergoing HA for displaced femoral neck fractures, all performed in a single health facility. The goal is to contribute to the limited existing evidence and provide trauma surgeons with realistic expectations when managing such complex cases.
Materials and Methods
After Institutional Review Board approval, a retrospective study was performed to evaluate all hemiarthroplasty patients. Using the procedural codes of surgery, a total of 2,477 HA cases were identified. All the cases had their clinical and radiographic data reviewed against our inclusion and exclusion criteria to extract the cases and data relevant to this study. The data collected included patients’ demographics, clinical information, and radiographic evaluation. Detailed information about the follow-up and postoperative clinical course was collected for all cases.
Inclusion Criteria
- Patients who underwent HA for a hip fracture, either primarily after trauma or for management of femoral neck fracture non-union.
- Patients who had a body mass index of 40 kg/m² or more at the time of surgery. Exclusion Criteria
- Patients without clinical follow-up notes after HA surgery.
- Patients with irrelevant surgical procedures or treatment modalities that shared the same recorded diagnoses.
Statistical Analysis
Descriptive statistical analysis was conducted using Microsoft Excel, version 2507 (Microsoft Corporation, Redmond, Washington, USA). The mean values, ranges, standard deviation, proportions, and percentages were calculated to present estimates about the outcomes.
Results
A total of 36 cases (35 patients) with BMI≥40 who underwent HA for femoral neck fractures or comminuted intertrochanteric fractures were retrieved from our database. Of these patients, 25 were female and 10 were male, with a mean age of 72.6 years (range: 52–91) at the time of primary HA (index) surgery. One female had bilateral femoral neck fractures, which occurred 83 months apart. Fifteen patients had chronic kidney disease (one had end-stage renal disease), twelve were hypothyroid, 10 were diabetic, and 8 had heart failure of variable degrees. The mean body mass index (BMI) for all patients at the time of surgery was 45.6 (range: 40.06-68.24) kg/m². Ten patients were previous smokers; one patient was an active smoker at the time of surgery, while the remaining patients were non-smokers.
The surgical procedures were performed by 29 different surgeons. The decision to perform HA, rather than THA, was based on the surgeon’s assessment, considering the patient’s age, activity levels, and functional status, and after agreement with the patient and their caregivers. Twenty-two cases were treated with bipolar HA, and 14 cases were treated with unipolar HA. Twenty-seven cases received cemented stems, and 9 received cementless stems. Thirty-three cases received standard stems, and three received long stems. The posterolateral approach was utilized in 31 cases, and the direct lateral approach was utilized in 5 cases. Postoperatively, all patients were routinely instructed to “weightbearing as tolerated”. Patients were instructed to undergo clinical and radiographic follow-up 6 weeks postoperatively (Figures 1,2), then as needed. The average radiographic and clinical follow-ups for all cases were 16 and 43.28 months.
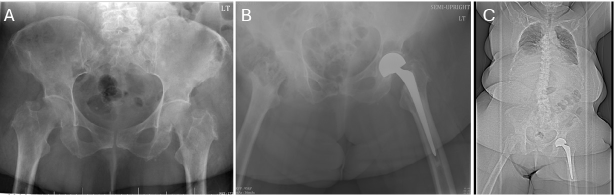
Figure 1: A) Plain pelvis radiograph showing a left sub capital femoral neck fracture in a 62-year-old female with a BMI of 54.87. B) Immediate postoperative (post-op) plain pelvis radiograph showing a cemented bipolar HA. C) A CT-scout 2 years post-op showing stable HA components. Note the soft tissue shadow in all images, indicating extreme obesity.
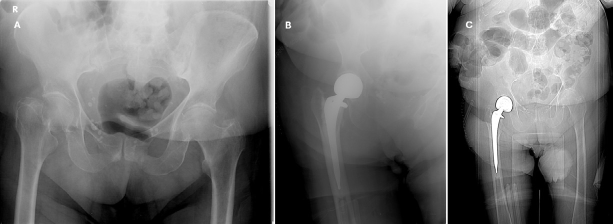
Figure 2: A) Plain pelvis radiograph showing a right trans cervical femoral neck fracture in a 91-year-old female with a BMI of 68.23. B) Immediate postoperative plain pelvis radiograph showing a cemented bipolar HA. C) A CT-scout showing stable HA components. Note the soft tissue shadow in all images, indicating extreme obesity. Note also the different obesity patterns from the patient in Figure 1.
Complications
Prosthetic joint infections
Five cases (13.9%) developed wound complications. Four cases (11.1%) suffered periprosthetic joint infections. Patients were 4 females with a mean age of 64.5 years at the time of surgery. Two cases had cemented bipolar and two had cemented unipolar HA. Three patients were diabetic. The eventual outcomes in the 4 cases were successful debridement and implant retention (1 case), a Girdlestone procedure (1 case), early mortality (one patient), and an articulating antibiotic spacer (one case). The PJI case summary was presented in Table 1. One more patient, a 75-year-old female, developed prolonged wound swelling and bloody discharge from the first day postoperative and underwent wound debridement and hematoma evacuation 6 days later. Bacterial cultures showed no bacterial growth, and the patient has been alive for 87 months till the present.
|
Case, age |
Clinical comorbidities |
Presentation/time after HA surgery |
Time of debridement surgery |
Management details |
Outcome |
Follow up |
|
1: 71years old |
-BMI 50.4 - Diabetes Mellitus (DM) -Hypothyroidism - Chronic kidney disease (CKD) -Heart failure -Gout |
Persistent wound discharge from day 1 post-op. |
14th and 21st day after HA surgery |
Underwent 2 surgical debridement procedures. |
Enterobacter species |
The patient lived for 29.8 months and then expired due to unrelated causes. |
|
2: 64-yearold |
-End stage renal disease -DM -BMI 45.2 -Myelodysplasia |
Persistent hip pain and wound discharge from the surgery day. |
21st day after HA surgery |
Surgical debridement and modular head exchange. Persistent wound discharge, re-debridement with resection arthroplasty (Girdlestone), followed by 2 sessions of wound debridement and wound VAC until wound healing. |
Morganella morganii |
The patient has been alive for 30 months. |
|
3: 71 years old |
-Chronic liver disease -Psoriasis -DM -CHF -Hypothyroidism -CKD -BMI 45.2 |
Persistent wound discharge from the surgery day. |
Patient received wound VAC postoperatively, then underwent surgical debridement on the 28th and 34th days post-op. |
Underwent 2 surgical debridement procedures. |
Staphylococcus species (blood culture) |
The patient died 1 week after the second surgical debridement with septicemia and multi-organ failure. |
|
4: 53 years old (Figure 4) |
-Hypothyroidism -CKD -Recurrent lower GIT infections -BMI 40.42 |
Persistent hip pain, acetabular erosion and elevated inflammatory markers 40 months after the HA surgery |
48 months after the HA surgery, the patient underwent surgical debridement and implant removal with articulating spacer insertion. |
Surgical debridement, implant removal, and articulating spacer insertion followed by 2 sessions of surgical debridement. |
Multi-organism infection (Proteus, Klebsiella and Staphylococcus species. |
The patient lived for approximately 20 months after the spacer insertion then died from chest infection. |
Table 1: Summary of the case presentations of the 4 infection cases.
Other Complications
One patient developed bilateral femoral deep venous thrombosis 8 months after the index HA surgery due to limited weight bearing and was managed with anticoagulants. One patient developed a contralateral proximal humeral fracture 6 years after the index HA surgery and was successfully managed conservatively. One patient underwent a contralateral total knee arthroplasty (TKA) 6 years after the index surgery and developed prosthetic knee joint infection that was managed with two-stage revision TKA. The same patient developed a surgical wound infection and exposed hardware of a contralateral (same side of the TKA, within the time of presentation of infected TKA) ankle fracture fixation that was performed 4 years before the HA surgery and was managed surgically by wound irrigation and implant removal. One patient sustained a fall 2 months after the index HA and developed stem subsidence, which was managed with revision to total hip arthroplasty. None of the patients developed periprosthetic fractures, dislocations, or primary acetabular erosion.
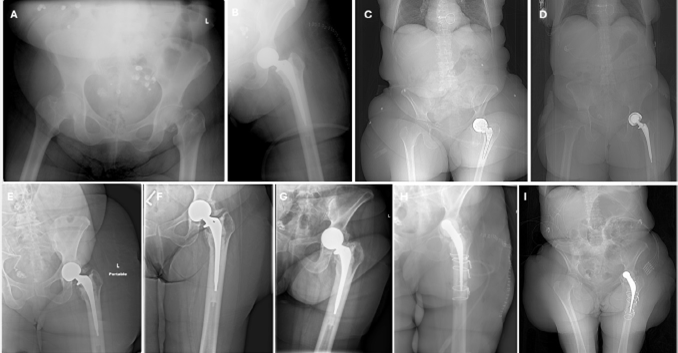
Figure 3: A) Plain pelvis radiograph showing a right sub capital femoral neck fracture in a 53-year-old female with a BMI of 40.42. B) Immediate postoperative plain pelvis gradiograph showing a cemented bipolar HA. C-E) Serial plain radiographs and CT scout taken at 9-, 19-, and 20-months post-op showing stable HA components. F) 40-month postoperative plain radiograph when the patient presented with hip pain showing acetabular protrusion. G) 48-month plain radiograph showing progressive protrusion. H) Immediate postoperative plain radiograph after HA revision to articulating spacer, performed 55 months after the index HA surgery. I) 55-month postop CT scout showing the articulating spacer. Note the soft tissue shadow in all images, indicating extreme obesity.
Mortality
Twenty-two patients (22/35 patients, 62.86%) died at a mean of 26.7 months (range: 0.06–76.7) after the primary HA surgery. Of them, six patients (17.14%) died within the first 3 months of the HA surgery. The median survival for all cases at the last follow-up or the date of death was 33.6 months. The 3-month, 1-year, and 3-year mortality for all patients was 17.14, 28.57, and 48.57%, respectively.
Discussion
This retrospective study investigates the outcomes of hip hemiarthroplasty for hip fractures in extremely obese patients. The outcomes indicate a particularly significant incidence of woundrelated complications (13.9%), including prosthetic joint infection (11.1%) and overall high early mortality (17.14% at 3 months). Other HA complications, such as instability, periprosthetic fractures and primary erosion [7], did not occur in any case of this series. The absence of instability and erosion in this series could be attributed to the overall limited weight-bearing and activities due to the high BMI, high mean age, relatively short clinical followup, and associated medical comorbidities.
Prosthetic joint infection after hemiarthroplasty is a devastating complication that is associated with high morbidity and mortality [13,22]. Its incidence largely varies in the literature, ranging from 1.7 to 7.3% [13], and it has been associated with up to 50% oneyear mortality [23,24]. Several risk factors for HA PJI have been identified. These include preoperative elements such as delayed surgery beyond one week, prolonged hospital stay, advanced age, female gender, obesity, prior surgical history, dementia, diabetes, immunosuppressive therapy (including corticosteroids), inadequate antibiotic prophylaxis, and concurrent infections caused by Staphylococcus aureus. Procedural and setting-related factors include surgeries performed by surgeons not specialised in hip fracture surgery, longer surgical and anaesthetic durations, the presence of two operating room staff members, and insufficient follow-up [25-30]. Postoperative risk factors encompass prolonged wound drainage, hematoma formation, hip dislocation, and repeated urinary catheterizations [25,31]. Among all, obesity is a significant risk factor for PJI after HA, particularly the latepresenting cases [25].
Obesity has been well known as a significant risk factor for poor outcomes, including wound-related complications and infections, in orthopedic trauma surgery [32,33] and arthroplasty [34,35]. In trauma surgery, obesity has been associated with increased rates of postoperative complications, longer hospital stays, and higher healthcare resource utilization. A retrospective study analyzing data from the National Trauma Data Bank found that morbidly obese patients with pelvic and acetabular fractures experienced significantly more overall complications, including deep surgical site infections (in operative acetabular or combined pelvic and acetabular fracture patients), and were more likely to require discharge to rehabilitation facilities [32].
Similarly, Childs et al [33] demonstrated that obese orthopedic trauma patients had an overall higher incidence of complications, including acute renal failure, soft tissue infections, ICU admission days, mechanical ventilation times, and total hospital stays. In total hip arthroplasty, A systematic review about the effect of obesity on THA found that obesity (BMI≥30) COULD BE associated with up to a four-fold increase in the incidence of complications, including dislocations, PJI after THA, compared to a BMI less than 30 [34], though the evidence remains conflicting. To note, increased obesity was found to further increase the risk of complications following THA. Warner et al [35] found that super obese patients (who have a BMI ≥ 50) had significantly higher rates of most complications than nonobese, obese, morbidly obese, and revision THA patients, including venous thromboembolism, infection, blood transfusion, medical complications, dislocation, readmission, and revision THA [35]. THA, however, differs from HA. The surgical settings and patient characteristics in HA, whose patients are mostly older and have more medical comorbidities, may render HA associated with a higher incidence of PJI than THA (up to 7.3% PJI risk in HA compared to up to 2.45% with primary THA) [13,36].
The evidence behind the outcomes of HA in obese patients remains seldom, with only one study, to our knowledge, existing [21]. In this study, De Genova et al [21] retrospectively reviewed 157 patients who underwent hip hemiarthroplasty (HA) or total hip arthroplasty (THA) for isolated femoral neck fractures and categorized them as obese or non-obese based on their BMI. The authors found that obesity was associated with increased operative times. In the HA group, obesity correlated with significantly longer operative times and showed a non-significant trend toward increased total operating room time and anaesthesia duration. In the THA group, obesity was significantly associated with longer operative times, total operating room time, and anaesthesia duration. The authors, however, did not find significant differences in postoperative complication rates between obese and non-obese patients in either surgical group, which may be attributed to the wide range of BMI that can fall under the umbrella of obesity and the relatively small sample size in this study.
In our study, the incidence of established PJI is 11.1%, which is significantly higher than the recorded incidence of PJI following HA (up to 7.3%) [13]. The higher incidence of PJI in our study may be attributed to the specific analysis of extremely obese patients, the higher incidence of associated medical comorbidities in such obese patients, and the high mean age in our study.
Obesity is a major global health challenge with profound implications for both individual well-being and national economies. It is associated with increased risks for numerous chronic conditions, including cardiovascular disease, type 2 diabetes, certain cancers, and musculoskeletal disorders, all of which contribute to reduced quality of life and premature mortality. Economically, obesity imposes a substantial burden on healthcare systems; in the United States alone, obesity-related medical costs were estimated at nearly $173 billion annually, with additional billions lost due to reduced productivity and absenteeism. The World Health Organization emphasizes that obesity affects all age groups and socioeconomic strata, and its rising prevalence threatens progress toward global health and development goals. Addressing obesity requires coordinated public health strategies that integrate prevention and management across all levels of care [37-39].
It is important to identify the implications of obesity in various health disciplines to set realistic expectations and increase patients’ and surgeons’ awareness of these complications. With the observed high incidence of prosthetic joint infections (11.1%) and the significant morbidity, mortality, and complexity of managing PJIs [40], especially when converting hemiarthroplasty (HA) to total hip arthroplasty [41], the implementation of enhanced infectioncontrol measures in extremely obese patients is imperative. Even though substantial weight loss is unfeasible in the acute trauma setting, strategies to mitigate infection risk should include optimized perioperative protocols, such as tailoring antibiotic prophylaxis by administering weight-based or higher-dose antibiotics (e.g., double-dose cefuroxime or cefazolin) for patients over 80 kg to ensure adequate tissue concentrations, strict adherence to standardized pre-incision timing and redosing intervals, ideally within 60 minutes and guided by pharmacokinetics, the use of comprehensive perioperative bundles including skin antisepsis, MRSA/MSSA decolonization when applicable, maintenance of normothermia, glycaemic control, and aseptic technique, and multidisciplinary coordination among surgeons, anaesthesiologists, nursing teams, and infection prevention specialists to foster a culture of safety [42-45]. Nevertheless, complication risks should be reasonably presented to the patients and their caregivers to achieve satisfactory outcomes.
This study is subject to several limitations. Foremost, its retrospective and non-comparative design inherently increases the risk of bias and restricts the strength of evidence that can be drawn from the findings. Additionally, the small sample size, stemming from the highly specific patient population, posed a significant constraint, limiting the feasibility of robust statistical analysis. Ideally, a larger, comparative study evaluating outcomes of hip hemiarthroplasty (HA) in obese versus non-obese patients would provide more definitive insights. Nevertheless, this is the first study to specifically examine the outcomes of HA in extremely obese individuals, marking an important step in addressing a gap in the literature. It lays the groundwork for future, larger-scale investigations.
Conclusion
Hip Hemiarthroplasty in extremely obese patients appears to be associated with a high incidence of prosthetic joint infections. However, the limited mobility often observed in this population may act as a protective factor against mechanical complications such as dislocation, periprosthetic fractures, and acetabular erosion, none of which were observed in this cohort. Further research is warranted to validate these findings and establish stronger evidence to guide clinical decision-making.
Conflicts of Interest
The authors declare no conflicts of interest.
Acknowledgements
Investigations were performed at Geisinger Medical Center, Danville, PA, USA.
Author Contributions
All authors contributed to this work.
Funding
This research did not receive funding.
Data Availability
Data can be requested from the corresponding author after fulfilling an institutional data use agreement.
Ethics Approval
The authors have received Institutional Review Board exemption based on 45 CFR 46, “Collection or Study of Existing Data,” considering the HIPPA Privacy Rule (45 CFR 160 and 164a) as it pertains to use and disclosure of protected health information.
References
- Beloosesky Y, Weiss A, Grinblat J, Brill S, Hershkovitz A (2004) Can functional status, after rehabilitation, independently predict long-term mortality of hip-fractured elderly patients? Aging Clin Exp Res 16: 448.
- Casadei R, Lughi M, Perini C, Maraldi M, Di Cecco F, et al (2025) Mortality risk factor in centenarians with proximal femoral fractures. Musculoskelet Surg 109:445-453.
- Koval KJ, Skovron ML, Aharonoff GB, Zuckerman JD (1998) Predictors of functional recovery after hip fracture in the elderly. Clin Orthop Relat Res 348: 22-8.
- Sofu H, Üçpunar H, Çamurcu Y, Duman S, Konya MN, et al (2017) Predictive factors for early hospital readmission and 1-year mortality in elder patients following surgical treatment of a hip fracture. Ulus Travma Acil Cerrahi Derg 23: 245-250.
- Camurcu Y, Cobden A, Sofu H, Saklavci N, Kis M (2017) What are the determinants of mortality after cemented bipolar hemiarthroplasty for unstable intertrochanteric fractures in elderly patients? J Arthroplasty 32: 3038-3043.
- Diamantopoulos AP, Hoff M, Skoie IM, Hochberg M, Haugeberg G (2013) Short- and long-term mortality in males and females with fragility hip fracture in Norway. A population–based study. Clin Interv Aging 8: 817-23.
- Mahmoud AN, Suk M, Horwitz DS (2024) Symptomatic Acetabular Erosion after Hip Hemiarthroplasty: Is It a Major Concern? A Retrospective Analysis of 2477 Hemiarthroplasty Cases. Journal of Clinical Medicine.13: 6756.
- Mahmoud AN, El-Husseini T, Elabd MA, Soliman RA, Maziad AM, (2024) Metastatic Hip Disease in the Elderly: Does Uncemented Hip Hemiarthroplasty have a Role?. SciBase Oncol 2:1015.
- Mahmoud AN, Doyle CM, Kline CM, Brule N, Sams KB, et al. (2024) Hip fracture in blind patients: Outcomes of hip hemiarthroplasty. Archives of Trauma Research. 13:209-215.
- Bourget-Murray J, Horton I, Morris J, Bureau A, Garceau S, et al (2022) Periprosthetic joint infection following hip hemiarthroplasty: factors associated with infection and treatment outcome Bone Jt Open. 3: 924-932.
- De Jong L, Klem TM, Kuijper TM, Roukema GR (2017) Factors affecting the rate of surgical site infection in patients after hemiarthroplasty of the hip following a fracture of the neck of the femur. The bone & joint journal. 99:1088-1094.
- Venishetty N, Jose J, Purudappa PP, Mounasamy V, Sambandam S (2024) Factors that influence the mortality of patients following hip hemiarthroplasty. Arthroplasty. 6: 36.
- Noailles T, Brulefert K, Chalopin A, Longis PM, Gouin F (2016) What are the risk factors for post-operative infection after hip hemiarthroplasty? Systematic review of literature. International orthopaedics. 40:1843-8.
- Ali H, Naik U, McDonald M, Almosa M, Horn K, et al. (2022) Complexities, complications of extreme obesity Autops Case Rep 12: e2021402.
- World Health Organization (WHO) (2022) Fact sheet: obesity and overweight. Geneva:
- Garrow JS, Webster J (1985) Quetelet’s index (W/H2) as a measure of fatness. Int J Obes. 9:147-53.
- National Institutes of Health (1998) Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Obes Res 6: 51S-209S.
- Medical Advisory Secretariat (2005) Bariatric surgery: an evidencebased analysis. Ont Health Technol Assess Ser 5: 1-148.
- Fryar CD, Carroll MD, Afful J (1960) Prevalence of overweight, obesity, and severe obesity among adults aged 20 and over: United States, 1960-1962 through 2017-2018. Washington, D.C.: NCHS Health E– Stats
- Zelle BA, Salazar LM, Howard SL, Parikh K, Pape HC (2022) Surgical treatment options for femoral neck fractures in the elderly. Int Orthop 46: 1111-1122.
- DeGenova DT, Passias BJ, Paulini AS, Myers PM, Dues B, Taylor BC (2024) The Effect of Obesity on Hemiarthroplasty and Total Hip Arthroplasty for Femoral Neck Fractures. J Long Term Eff Med Implants 34 :53-60.
- Mahmoud AN, Brule NR, Suk M, Horwitz DS (2025) Outcomes of Staphylococcal Prosthetic Joint Infection After Hip Hemiarthroplasty: Single Center Retrospective Study. Medicina (Kaunas). 61: 602.
- Rogmark C, Johnell O (2006) Primary arthroplasty is better than internal fixation of displaced femoral neck fractures: a meta-analysis of 14 randomized studies with 2,289 patients. Acta Orthop 77: 359-67.
- Edwards C, Counsell A, Boulton C, Moran CG (2008) Early infection after hip fracture surgery: risk factors, costs and outcome. J Bone Joint Surg Br 90: 770-777.
- Cordero-Ampuero J, de Dios M (2010) What are the risk factors for infection in hemiarthroplasties and total hip arthroplasties? Clin Orthop Relat Res 468: 3268-77.
- Ridgeway S, Wilson J, Charlet A, Kafatos G, Pearson A, Coello R (2005) Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg Br. 87: 844-50.
- Lau AC, Neo GH, Lee HC (2014) Risk factors of surgical site infections in hip hemiarthroplasty: a single-institution experience over nine years. Singapore Med J 55: 535-8.
- Acklin YP, Widmer AF, Renner RM, Frei R, Gross T (2011) Unexpectedly increased rate of surgical site infections following implant surgery for hip fractures: problem solution with the bundle approach. I njury. 42:209-16.
- Harrison T, Robinson P, Cook A, Parker MJ (2012) Factors affecting the incidence of deep wound infection after hip fracture surgery. J Bone Joint Surg Br 94: 237-240.
- Shah SN, Wainess RM, Karunakar MA (2005) Hemiarthroplasty for femoral neck fracture in the elderly surgeon, hospital volume-related outcomes. J Arthroplasty. 20: 503-508.
- Cumming D, Parker MJ (2007) Urinary catheterisation, deep wound infection after hip fracture surgery Int Orthop 31: 483-485.
- Carson JT, Shah SG, Ortega G, Thamyongkit S, Hasenboehler EA, Shafiq B (2018) Complications of pelvic and acetabular fractures in 1331 morbidly obese patients (BMI ≥ 40): a retrospective observational study from the National Trauma Data Bank. Patient Saf Surg. 12: 26.
- Childs BR, Nahm NJ, Dolenc AJ, Vallier HA (2015) Obesity Is Associated with More Complications and Longer Hospital Stays After Orthopaedic Trauma. J Orthop Trauma 29: 504-9.
- Haynes J, Nam D, Barrack RL (2017) Obesity in total hip arthroplasty:does it make a difference? B one Joint J 99-B(1_Supple_A): 31-36.
- Werner BC, Higgins MD, Pehlivan HC, Carothers JT, Browne JA (2017) Super obesity is an independent risk factor for complications after primary total hip arthroplasty. The Journal of arthroplasty. 32: 402-406.
- Zeng ZJ, Yao FM, He W, Wei QS, He MC (2023) Incidence of periprosthetic joint infection after primary total hip arthroplasty is underestimated: a synthesis of meta-analysis and bibliometric analysis. J Orthop Surg Res 18: 610.
- Centers for Disease Control, Prevention (2022) Adult obesity facts. U.S. Department of Health & Human Services.
- World Health Organization (2023) Obesity.
- Hartmann-Boyce J, Cobiac LJ, Theodoulou A, Oke JL, Butler AR, et al. (2023) Weight regain after behavioural weight management programmes and its impact on quality of life and cost effectiveness: Evidence synthesis and health economic analyses. Diabetes Obes Metab 25: 526-535.
- Ometti M, Delmastro E, Salini V (2022) Management of prosthetic joint infections: a guidelines comparison. Musculoskelet Surg 106: 219-226.
- Ansari S, Gupta T, Pranav J, Gupta K, Raja BS, et al. (2025) Outcome of hemiarthroplasty to total hip arthroplasty conversion: a systematic review. Musculoskelet Surg 109: 389-410.
- Hasler S, Unterfrauner I, Olthof MGL, Jans P, Betz M, et al. (2021) Deep surgical site infections following double-dose perioperative antibiotic prophylaxis in adult obese orthopedic patients. International Journal of Infectious Diseases. 108: 537-542.
- Stanford Health Care (2023) SHC Surgical Antimicrobial Prophylaxis Guidelines.
- Scottish Intercollegiate Guidelines Network (SIGN) (2022) Antibiotic Prophylaxis in Orthopaedic Surgery. Edinburgh: SIGN
- Association for Professionals in Infection Control and Epidemiology (APIC) & AORN (2023) Partnering with Perioperative Colleagues to Prevent Infection. Journal of Infection Prevention. 24: 145-150.