Totally Implantable Venous Access Port Via Nondominant Limb Cephalic Vein. Experience of A Single Surgeon
Article Type
Research Article
Online Date
March 16, 2026
Open Access
Yes
Angel Barba*
Angiology and Vascular Surgery Clinic, Bilbao, Spain
*Corresponding author: Angel Barba, Angiology and Vascular Surgery Clinic, Bilbao, Spain
Citation: Barba A (2025) Totally Implantable Venous Access Port Via Nondominant Limb Cephalic Vein. Experience of A Single Surgeon. Glob J Surg Surgical Res 1(1): 85-90.
Received Date: 17 May, 2025; Accepted Date: 02 June, 2025; Published Date: 05 June, 2025
Abstract
Introduction: The purpose of this study is to demonstrate that placement of the Totally Implantable Venous Access Port (TIVAP) via the cephalic vein (CV) is straightforward, with good success rates and few complications.
Methods: This is a longitudinal, descriptive and retrospective study analyzing the outcome of TIVAP implants by a single vascular surgeon in a private health center. CV dissection of the non-dominant limb is the chosen route in principle for placing the catheter after performing a preoperative Doppler ultrasound in an outpatient procedure.
Results: 596 TIVAPs were implanted in 578 patients, 382 of whom were female (66.1%), and the average age was 60 years (r=20-87). In 503 cases (84.4%) placement via the CV had a 97.4% success rate. There were no serious intraoperative complications, while there were 16 postoperative complications (3.2%). In 93 cases (15.6%), subclavian vein puncture was performed, with a success rate of 97.8%, resulting in 1 case (1.1%) of intraoperative and 3 cases of (3.2%) postoperative complications. There were no statistically significant differences.
Conclusions: The cephalic vein provides excellent access for TIVAP implantation, with a high success rate and minimal intra- and post-operative complications.
Keywords: Cephalic Vein; Preoperative Ultrasound; Venous Access Port
Introduction
In the 1970s, Broviacs ([1], 1973) and Hickman ([2], 1979) began to place partially implantable catheters, and later Niederhuber ([3], 1982) implanted the first Totally Implantable Venous Access Port-a-Cath (TIVAP) via the Cephalic Vein (CV). Since then, potential complications arising from the materials used, such as foreign body reaction, phlebitis, port fatigue, etc., have been gradually eliminated. For all these reasons, today many believe that it is essential to place a reservoir for prolonged chemotherapy in cancer patients. TIVAP implantation is usually performed using the Seldinger technique via the right subclavian vein (SV) or jugular vein (JV), with subsequent placement of the port in the anterior thorax. This technique is straightforward for experienced surgeons to perform but it has the disadvantage of potential intra- and postoperative complications. Given that in 2013 it was estimated that 89.5-90% of people in Spain were right-handed, and in light of my time as resident in the Department of Cardiovascular and Thoracic Surgery at the Hospital of Basurto, where placement of pacemaker electrodes was performed via the left CV with few complications, I decided to perform TIVAP implants via the CV of the non-dominant extremity as the primary route. The aim of this paper is to present the results of this technique and compare them with those presented by other authors.
Methods
Between 1 January 2009 and 31 December 2016, a single Angiologist and Vascular Surgeon placed 596 TIVAPs for cancer patient chemotherapy at the San Sebastián/Zorrotzaurre Units attached to the Igualatorio Medical-Surgical Clinic in Bilbao (Vizcaya). The patient’s affiliation, together with their personal and medical history were collected during consultation using a FileMaker 10 database. Similarly, the surgical technique was explained to the patients, informed consent was requested, and they were provided a guide on TIVAP implants and maintenance drawn up by the vascular surgeon and nurses from the Oncology Outpatient Hospital (OOH). In addition to physical examination, Doppler ultrasound (Esaote-MyLab50) of the cephalic-axillary-subclavian venous axis was performed to assess the diameter and patency of the CV. When found to be not suitable, the TIVAP was implanted directly by puncture of the SV.
On an outpatient basis and employing local anesthesia in the operating room (specifically mepivacaine 2%), an incision was made in the left deltopectoral groove. In left-handed patients, those with a prior TIVAP implantation in this area, or left-sided breast surgery patients who had undergone lymphadenectomy, access was chosen via the right CV. The CV was dissected, distally ligated and an HP® NuPort (PHS MEDICAL) catheter device was placed without the guidewire or the dilator included in the kit. Using fluoroscopic monitoring with a Philips BV Pulsera CV-Arm, the placement of the distal end at the confluence between the superior vena cava and the right atrium was verified ("the catheter tip is dancing"), after which the CV was ligated proximally to secure the catheter. When it was not possible to use this method, access to the SV was made using the Seldinger technique, but in this case a 4F standard Micro-Introducer Kit (Angio Dinamics) needle and micro-inducer were used initially to cannulate the vein. Once the vein was cannulated and the sheath introducer was placed in the SV, the reservoir guidewire from the kit was inserted and the procedure was performed in the standard manner.
A subcutaneous pocket was created, the catheter was attached to the port and cut, the port was placed in its chamber, and it was always fixed to the muscle wall at one or more of the port side holes using 3-0 Prolene. Adequate TIVAP functioning was verified and the subcutaneous tissue and skin were then closed following the standard procedure. A final check of system patency was performed, and the entire device was sealed with a heparinized saline solution. Antibiotic prophylaxis was not performed. When appropriate, the patient's TIVAP was left cannulated for immediate use in the OOH. After use, either for drug infusion or blood samples, the TIVAP was sealed with 10 cc of saline solution and 5-ml of Fibril in (Heparin Na 20 IU/ml) from ROVI Laboratories, reapplied once every 2.5 months until the oncologist decided to discontinue. This work was done by the nurses at the OOH. The various routes, duration of surgery, complications, TIVAP removal and its causes and patient survival were examined. Complications are defined as intraoperative if they occurred in the operating room or within the first 12 hours, postoperative if they occurred after 12 hours but within the first 30 days after the intervention and late if they occurred at a later time. A slight postoperative hematoma (blood suffusion) was not considered a serious complication. The established criteria for TIVAP removal include completion of treatment, systemic infection or sepsis that could not be resolved with antibiotic treatment and/or intolerable neuralgia. Descriptive statistical analysis of the data was performed using R Commander software (www.rcommander.com). Mean values and standard deviations are presented for continuous variables. In order to compare proportions, hypothesis testing was performed using the Mid-p exact test using the Open Epi software program (www.openepi.com).
Results
During the study period, 596 TIVAP were implanted in 578 patients, of whom 586 (98.3%) were on an outpatient basis and 10 (1.7%) were hospitalized patients. Three-hundred and eighty-two patients (66.1%) were female and 196 (33.9%) were male. The overall average age was 60.1 years (r=20-87). Neoplasm distribution is shown in (Table 1).
|
Male (n= 196) |
Female (n=382) |
Total (n=578) |
|
|
Breast |
- |
211 (55.2%) |
211 (36.6%) |
|
Colon |
97 (49.5%) |
92 (24.1%) |
189 (32.7%) |
|
Lung |
29 (14.8%) |
21 (5.5%) |
50 (8.7%) |
|
Gynecological |
- |
34 (8.9%) |
34 (5.9%) |
|
Pancreas |
15 (7.6%) |
5 (1.3%) |
20 (3.5%) |
|
Mouth |
12 (6.1%) |
1 (0.3%) |
13 (2.2%) |
|
Urological |
12 (6.1%) |
1 (0.3%) |
13 (2.2%) |
|
Larynx |
10 (5.2%) |
- |
10 (1.7%) |
|
Esophagus |
9 (4.6%) |
1 (0.3%) |
10 (1.7%) |
|
Others |
12 (6.1%) |
16 (4.2%) |
28 (4.8%) |
Table 1: Types of neoplasm in the series.
with breast neoplasms being the most common among women (55.2%) and colon neoplasms the most common among men (49.5%).Five-hundred and twenty-two TIVAPs (87.6%) were implanted on the left side and among the 74 cases (12.4%) for which it was initially decided to implant on the right side, 42 cases (56.8%) were related to left breast surgery and/or lymphadenectomy, 14 (18.9%) to neoplasm recurrence with prior TIVAP placement on the left side, 8 (10.8%) to left-handed patients, 5 (6.8%) to left brachiocephalic vein occlusion by metastatic compression, 2 (2.7 %) to left TIVAP infection and 3 cases (4.1%) were due to other reasons. Of the 596 deltopectoral grooves explored preoperatively by Doppler ultrasound, the CV was found initially suitable for TIVAP implantation in 519 cases (87.1%), while in 77 patients (12.9%) the CV was not located, was thrombosed or was hypoplastic, requiring SV implantation for these patients. This resulted in an overall left CV success rate of 97.4% after clinical ultrasound screening and 98.6% for left SV (Figure 1).
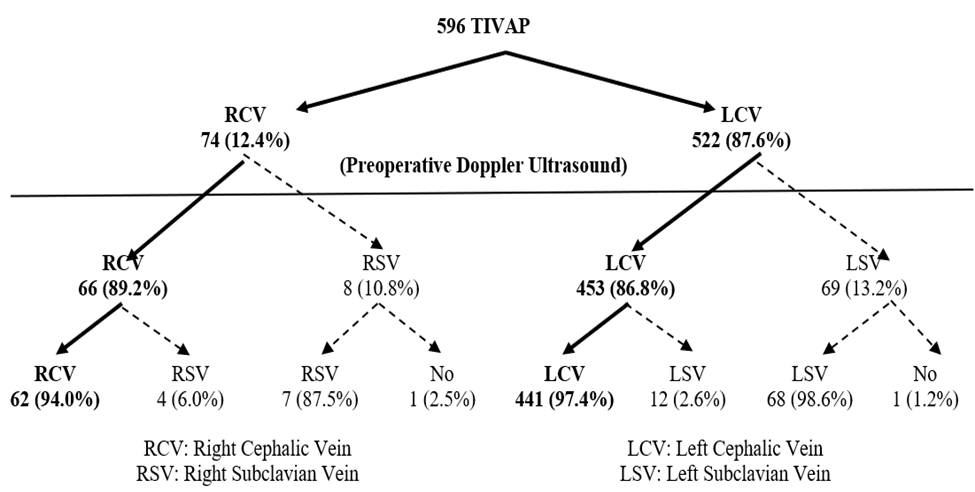
Figure 1: TIVAP distribution.
There was no significant difference between them (p=0.62). The CV could not be cannulated in 2 patients. The mean operating time when the CV was used was 25 minutes (r=20-39) and 20 minutes via the SV (r=15-33). There were also no significant differences (p =0.71) between them.
Overall, severe complications occurred in 16 cases (3.2%) via the CV and 4 (4.4%) via the SV. No serious intraoperative complications occurred when the CV route was used, whereas when the SV was cannulated, pneumothorax occurred in 2.4% of cases. There were no vascular or nervous system injuries (Table 2).
|
CV (n=503) |
SV* (n=91) |
p |
|
|
Intraoperative (<12 hours) - Pneumothorax |
0 (0.0%) - |
1 (1.1%) 1 |
NS (p=0.15) |
|
Postoperative (<30 days) - Hematoma - Deep vein thrombosis - Neuralgia |
9 (1.8%) 2 4 3 |
2 (2.2%) - 2 - |
NS (p=0.75) |
|
Late (>30 days) - Deep vein thrombosis - TIVAP infection - Skin erosion |
7 (1.4%) 1 5 1 |
1 (1.1%) - 1 - |
NS (p=0.91) |
|
Total |
16 (3.2%) |
4 (4.4%) |
NS (p=0.55) |
(*) The TIVAP could not be implanted in two cases. CV: Cephalic Vein; SV: Subclavian Vein
Table 2: Complications related to the chosen access route.
shows all complications observed during the study. The most frequent were 7 cases (1.2%) of deep venous thrombosis (DVT) in the ipsilateral limb that were treated with LMWH and did not require TIVAP removal, as well as systemic infection in 6 cases (1.0%). Three patients (0.5%) had persistent neuralgia when the CV was used for the implant, and one port decubitus (0.2%). During the study, there was no catheter fracture or migration, or port inversion. There were no significant differences globally (p=0.55) or between the different complications. One-hundred and eight TIVAP were explanted (18.1%), 98 (16.4%) due to completion of treatment at a mean of 872 days after implant (r=105-3381), 5 (0.8%) due to post-puncture infection at a mean of 664 days (r=151-1351), 3 (0.5%) due to medically intractable neuralgia at a mean of 110 days (r=70-173) and 2 (0.3%) due to other causes at a mean of 830 days (r=215-2995). Three hundred and forty-four patients completed the study (57.7%) while 249 died (41.8%), with an average follow-up of 1245 days (r=1-4002) and 513 days (r=35-2753), respectively. Three patients were lost to follow-up during the study (0.5%).
Discussion
Regarding the surgical technique, introduction of the TIVAP catheter via CV dissection is justified by the avoidance of major intraoperative complications from venipuncture (hemo/pneumothorax, arterial or plexus injury), which in recent studies range between 0.5 and 6% [4]. With this technique, these complications are negligible, as is the case in our study. Placement is preferable on the left side due to the higher proportion of right-handed persons; that way, the catheter will undergo fewer displacements, given the decreased daily motility of the non-dominant limb [5]. A concern of using the left side might be the use of automobile seat belts and the potential compression of the port, but because it is implanted in the anterior-external pectoralis area, the possibility of compression is effectively zero. Surgical intervention is performed under local anesthesia, as practiced by many other groups [6], though some highly-published authors advocate general anesthesia [7]. The use of antibiotic prophylaxis is a hotly debated topic. It was not used for this paper, although serious precautionary aseptic measures were taken during implantation. Moreover, studies from multiple clinics show that prophylaxis is not necessary [8], but in everyday practice, each surgeon will decide to use it or not depending on his or her results. Numerous studies claim that the implant success rate is much higher when performing venipuncture rather than dissection, 71% versus 90%, as Nocito [9] states, but when preoperative Doppler ultrasound is performed to eliminate instances of CV absence, hypoplasia and possible abnormalities prior to surgery, the surgical success rate is similar to that of the outcomes published when puncturing the SV [10]. The success rate is 96.9% for the methods presented in this paper.
One notable aspect regarding CV TIVAP implantation is that the catheter is proximally fixed to the CV by ligation, thus preventing possible migration following a possible break at the catheter/port junction [5,11]. Furthermore, introducing the catheter through the CV avoids the trauma of SV puncture and the potential microtraumas caused by it in the clavicle/1st rib space, especially when implanting in the dominant limb. Across this series of interventions, there were no ruptures or migrations. One complication that occurred during the initial cases was that, while ligating the CV, some branch of the brachial plexus was also ligated, resulting in intense pain that forced removal of the TIVAP in our case. Another published complication relating to the surgical technique is the rotation of the port which may occur in up to 0.6% of cases [12]. However, none occurred over the course of this study, quite possibly because we fixed the port to the anterior pectoralis major wall at 2 locations. Regarding operating times, this varies between 17 and 45 minutes [4,13] in recent literature when accessing via the CV. In this study, the mean time spent was 25 minutes. In his study, Biffi [14] describes the incidence of DVT in TIVAP implantation, which ranges from 27% to 66% in its asymptomatic form and 0.3% to 28.3% in symptomatic cases, stressing that venipuncture increases the incidence of DVT. When the CV route is used, the incidence of DVT varies between 4.4% and 8.3% [6,14], which in our case amounted to 1.1%. It should be stressed that the presence of DVT does not necessarily require TIVAP removal because, according to most authors, anticoagulant therapy is sufficient to resolve it. Moreover, it should be noted that neoplastic disease itself is a risk factor for the occurrence of DVT.
The greatest systemic risk is infection. During the immediate postoperative period, as previously mentioned, antibiotic prophylaxis does not solve the problem of infection, and subsequently during TIVAP use, I believe that painstaking care when using the system is the foundation for preventing infection around the port, currently estimated at between 2.6 and 9.0% of cases [15]. In this study, the 1.1% incidence is possibly due to the thorough and excellent care of the catheters by the nursing staff of our Clinic. In many cases, catheter infection is often associated with the decline in immunity from the neoplasm itself. But even so, the infection rate for the CV route stands at between 1.9% and 10.8% [13, 14]. In our hospital system, infection has led to TIVAP removal until now, but after a thorough review of recent literature, we will initiate a change in criteria and will employ specific antibiotic treatment as first choice in order to prevent removal.In the recent literature, the explant rate is 17-20% [16], and in most studies the highest percentage relates to completion of treatment (78% -90%), except in those cases [17] in which systemic infection is the leading cause for removal (46.2%). The results in this study are similar to those presented by the majority of other authors.
Conclusions
In conclusion, performing a preoperative Doppler ultrasound improves the success rate of TIVAP implantation via CV dissection in the non-dominant limb, similar to that obtained by SV puncturing, showing excellent results without serious intraoperative complications, such as pneumothorax, while the percentage of postoperative and long-term complications is similar or superior to those obtained via SV puncturing. Proper indication by the oncologist, proper surgical technique and painstaking TIVAP care by the nursing staff are the keys to positive results and higher patient satisfaction.
References
- BroviacJW, Cole JJ, Scribner BH (1973) A silicone rubber atrial catheter for prolonged parenteral alimentation. Surg Gynecol Obstet 136: 602-606.
- Hickman RO, Buckner CD, Clift RA, Sanders JE, Stewart P, et al. (1979) Modified right atrial catheters for access to the venous system in marrow transplant recipients. Surg Gynecol Obstet 148: 871-875.
- Niederhuber JE, Ensminger W, Gyves JW, Lipeman M, Doan K, et al. (1982) Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery 92: 706-712.
- Di Carlo I, Pulvirenti E, Mannino M, Toro A (2010) Increased percutaneous technique for totally implantable venous access devices. Is it real progress? A 27-year comprehensive review on early complications. Surg Oncol Ann 17: 1649-1656.
- Lin CH, Wu HS, Chan D, Hsieh CB, Huang MH, et al. (2010) The mechanisms of failure of totally implantable central venous access system: analysis of 73 cases with fracture of catheter. Eur J of Surg Oncol 36: 100-103.
- Barroso de Oliveira E, Aguiar M, Marques Avelar TM, VIEIRA SC (2013) Totally implantable central venous catheters for chemotherapy: experience with 793 patients. Rev Col Bras Cir 40: 186-190.
- Mudan S, Giakoustidis A Morrison D, Iosifidou S, Raobaikady R, et al. (2015) 1000 Port-A-Cath placements by subclavian vein approach: single surgeon experience. World J Surg 39: 328-334.
- Venkatesan AM, Kundu S, Sacks D, Wallace MJ, Wojak JC, et al. (2010) Practice guideline for adult antibiotic prophylaxis during vascular and interventional radiology procedures. J Vasc Interv Radiol 21: 1611-1630.
- Nocito A, Wildi S, Ru?bach K, Clavien P-A, Weber M (2009) Randomized clinical trial comparing venous cutdown with the Seldinger technique for placement of implantable venous access ports. Br J Surg 96: 1129-1134.
- Bif? R, Orsi F, Pozzi S, Pace U, Bonomo G, et al. (2009) Best choice of central venous insertion site for the prevention of catheter-related complications in adult patients who need cancer therapy: a randomized trial. Ann Oncol 2009.
- Barbetakis N, CHRISTOS Asteriou C, Kleontas A, Tslikas C (2001) Totally Implantable Central Venous Access Ports. Analysis of 700 Cases. J Surg Oncol 104: 654-656.
- Wildgruber M, Borgmeyer S, Haller B, Jansen H, Gaa J, et al. (2015) Short-term and long-term outcome of radiological-guided insertion of central venous access port devices implanted at the forearm: a retrospective monocenter analysis in 1704 patients. Eur Radiol 25: 606-616.
- Granziera E, Scarpa M, Ciccarese A, Filip B, Cagol M, et al. (2014) Totally implantable venous access devices: retrospective analysis of different insertion techniques and predictors of complications in 796 devices implanted in a single institution. BMC Surgery 14: 27.
- Biffi R, Toro A, Pozzi S, Di Carlo I (2006) Totally implantable vascular access devices 30 years after the first procedure. What has changed and what is still unsolved? Support Care Cancer 22: 1705-1714.
- Cil BE, Canyi M, Peynircio B, Hazirolan T, Carkaci S, et al. (2006) Subcutaneous venous port implantation in adult patients: a single center experience. Diagn Interv Radiol 12: 93-98.
- Shim J, Seo TS, Song MG, Cha IH, Kim JS, et al. (2014) Incidence and risk factors of infectious complications related to implantable venous-access ports. Korean J Radiol 15: 494-500.
- Fischer L, Knebel L, Schroder S, Bruckner T, Diener MK, et al. (2008) Reasons for explantation of totally implantable access ports: a multivariate analysis of 385 consecutive patients. Ann Surg Oncol 15: 1124-1129.